Other Names: Bowel incontinence,Fecal incontinence
Description:
Bowel incontinence is the loss of bowel control, leading to an involuntary passage of stool. This can range from occasionally leaking a small amount of stool and passing gas, to completely losing control of bowel movements…..CLICK & SEE
You have a bowel control problem if you accidentally pass solid or liquid stool or mucus from your rectum.* Bowel control problems include being unable to hold a bowel movement until you reach a toilet and passing stool into your underwear without being aware of it happening. Stool, also called feces, is solid waste that is passed as a bowel movement and includes undigested food, bacteria, mucus, and dead cells. Mucus is a clear liquid that coats and protects tissues in your digestive system.
Among people over age 65, most surveys find that women experience bowel incontinence more often than men. One to three out of every 1,000 women report a loss of bowel control at least once per month.
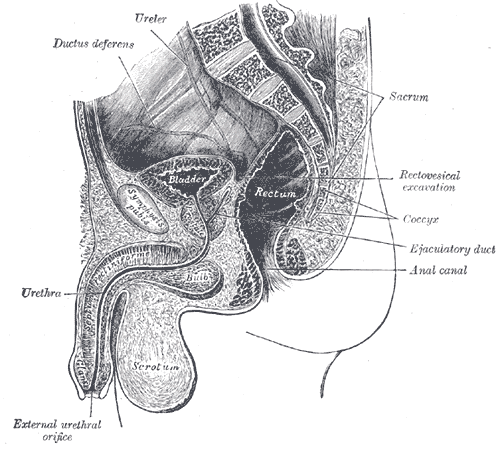
To hold stool and maintain continence, the rectum, anus, pelvic muscles, and nervous system must function normally. You must also have the physical and mental ability to recognize and respond to the urge to have a bowel movement.
Ringlike muscles called sphincters close tightly around your anus to hold stool in your rectum until you’re ready to release the stool. Pelvic floor muscles support your rectum and a woman’s vagina and also help with bowel control.
Causes:
Bowel control problems are often caused by a medical issue and can be treated.
*Chronic constipation, causing the muscles of the anus and intestines to stretch and weaken, and leading to diarrhea and stool leakage (see: encopresis)
*Chronic laxative use
*Colectomy or bowel surgery
*Decreased awareness of sensation of rectal fullness
*Emotional problems
*Gynecological, prostate, or rectal surgery
*Injury to the anal muscles due to childbirth (in women)
*Nerve or muscle damage (from trauma, tumor, or radiation)
*Severe diarrhea that overwhelms the ability to control passage of stool
*Severe hemorrhoids or rectal prolapse
*Stress of unfamiliar environment
*A disease or injury that damages your nervous system
*Poor overall health from multiple chronic, or long lasting, illnesses
*A difficult childbirth with injuries to your pelvic floor—the muscles, ligaments, and tissues that support your uterus, vagina, bladder, and rectum
Diagnosis:
To diagnose what is causing your bowel control problem, your doctor will take your medical history, including asking the questions listed in “What do I tell my doctor about my bowel control problem?” Your doctor may refer you to a specialist who will perform a physical exam and may suggest one or more of the following tests:
* anal manometry
* anal ultrasound
* magnetic resonance imaging (MRI)
* defecography
* flexible sigmoidoscopy or colonoscopy
* anal electromyography (EMG)
Anal manometry. Anal manometry uses pressure sensors and a balloon that can be inflated in your rectum to check how sensitive your rectum is and how well it works. Anal manometry also checks the tightness of the muscles around your anus. To prepare for this test, you should use an enema and not eat anything 2 hours before the test. An enema involves flushing water or a laxative into your anus using a special squirt bottle. A laxative is medicine that loosens stool and increases bowel movements. For this test, a thin tube with a balloon on its tip and pressure sensors below the balloon is put into your anus. Once the balloon reaches the rectum and the pressure sensors are in the anus, the tube is slowly pulled out to measure muscle tone and contractions. No sedative is needed for this test, which takes about 30 minutes.
Anal ultrasound. Ultrasound uses a tool, called a transducer, that bounces safe, painless sound waves off your organs to create an image of their structure. An anal ultrasound is specific to the anus and rectum. The procedure is performed in a doctor’s office, outpatient center, or hospital by a specially trained technician, and the images are interpreted by a radiologist—a doctor who specializes in medical imaging. A sedative is not needed. The images can show the structure of your anal sphincter muscles.
MRI. MRI machines use radio waves and magnets to produce detailed pictures of your internal organs and soft tissues without using x rays. The procedure is performed in an outpatient center or hospital by a specially trained technician, and the images are interpreted by a radiologist. A sedative is not needed, though you may be given medicine to help you relax if you have a fear of confined spaces. An MRI may include the injection of special dye, called contrast medium. With most MRI machines, you lie on a table that slides into a tunnel-shaped device that may be open ended or closed at one end; some newer machines are designed to allow you to lie in a more open space. MRIs can show problems with your anal sphincter muscles. MRIs can provide more information than anal ultrasound, especially about the external anal sphincter.
Defecography. This x ray of the area around your anus and rectum shows whether you have problems with
* pushing stool out of your body
* the functioning of your anus and rectum
* squeezing and relaxing your rectal muscles
The test can also show changes in the structure of your anus or rectum. To prepare for the test, you perform two enemas. You can’t eat anything for 2 hours before the test. During the test, the doctor fills your rectum with a soft paste that shows up on x rays and feels like stool. You sit on a toilet inside an x-ray machine. The doctor will ask you to first pull in and squeeze your sphincter muscles to prevent leakage and then to strain as if you’re having a bowel movement. The radiologist studies the x rays to look for problems with your rectum, anus, and pelvic floor muscles.
Flexible sigmoidoscopy or colonoscopy. These tests are similar, but a colonoscopy is used to view your rectum and entire colon, while a flexible sigmoidoscopy is used to view just your rectum and lower colon. These tests are performed at a hospital or outpatient center by a gastroenterologist—a doctor who specializes in digestive diseases. For both tests, a doctor will give you written bowel prep instructions to follow at home. You may be asked to follow a clear liquid diet for 1 to 3 days before either test. The night before the test, you may need to take a laxative. One or more enemas may be needed the night before and about 2 hours before the test.
In most cases, you will be given a light sedative, and possibly pain medicine, to help you relax during a flexible sigmoidoscopy. A sedative is used for colonoscopy. For either test, you will lie on a table while the doctor inserts a flexible tube into your anus. A small camera on the tube sends a video image of your bowel lining to a computer screen. The test can show problems in your lower GI tract that may be causing your bowel control problem. The doctor may also perform a biopsy, a procedure that involves taking a piece of tissue from the bowel lining for examination with a microscope. You won’t feel the biopsy. A pathologist—a doctor who specializes in diagnosing diseases—examines the tissue in a lab to confirm the diagnosis.
You may have cramping or bloating during the first hour after these tests. You’re not allowed to drive for 24 hours after a colonoscopy or flexible sigmoidoscopy to allow the sedative time to wear off. Before the test, you should make plans for a ride home. You should recover fully by the next day and be able to go back to your normal diet.
Anal EMG. Anal EMG checks the health of your pelvic floor muscles and the nerves that control your muscles. The doctor inserts a very thin needle wire through your skin into your muscle. The wire on the needle picks up the electrical activity given off by the muscles. The electrical activity is shown as images on a screen or sounds through a speaker. Another type of anal EMG uses stainless steel plates attached to the sides of a plastic plug instead of a needle. The plug is put in your anus to measure the electrical activity of your external anal sphincter and other pelvic floor muscles. The test can show if there is damage to the nerves that control the external sphincter or pelvic floor muscles by measuring the average electrical activity when you
* relax quietly
* squeeze to prevent a bowel movement
* strain to have a bowel movement
Treatment:
Home Care:
Incontinence is not a hopeless situation. Proper treatment can help most people, and can often eliminate the problem.
Treating bowel incontinence should begin by identifying the cause of the incontinence. There are several ways to strengthen the anal and pelvic muscles and promote normal bowel function.
Rutine pelvic floor exercise may improve the condition.
FECAL IMPACTION:
Fecal impaction is usually caused by chronic constipation. It leads to a mass of stool that partially blocks the large intestine. If constipation or fecal impaction contributes to fecal incontinence, usually laxatives and enemas are of little help. A health care provider may need to insert one or two fingers into the rectum and break the mass into smaller pieces that can pass more easily.
Take measures to prevent further fecal impaction. Add fiber to your diet to help form normal stool. Use other medications your health care provider recommends. In addition, drink enough fluids and get enough exercise to enhance normal stool consistency.
DIET:
Bowel incontinence often occurs because the rectal sphincter is less able to handle large amounts of liquid stool. Often, simply changing the diet may reduce the occurrence of bowel incontinence.
Certain people develop diarrhea after eating dairy foods because they are unable to digest lactose, a sugar found in most dairy products. Some food additives such as nutmeg and sorbitol may cause diarrhea in certain people.
Adding bulk to the diet may thicken loose stool and decrease its amount. Increasing fiber (30 grams daily) from whole-wheat grains and bran adds bulk to the diet. Psyllium-containing products such as Metamucil can also add bulk to the stools.
Formula tube feedings often cause diarrhea and bowel incontinence. For diarrhea or bowel incontinence caused by tube feedings, talk to your health care provider or dietitian. The rate of the feedings may need to be changed, or bulk agents may need to be added to the formula.
Eating, Diet, and Nutrition:
Changes in your diet that may improve your bowel control problem include
*Eating the right amount of fiber. Fiber can help with diarrhea and constipation. Fiber is found in fruits, vegetables, whole grains, and beans. Fiber supplements sold in a pharmacy or health food store are another common source of fiber to treat bowel control problems. The Academy of Nutrition and Dietetics recommends getting 20 to 35 grams of fiber a day for adults and “age plus five” grams for children. A 7-year-old child, for example, should get “7 plus five,” or 12, grams of fiber a day. Fiber should be added to your diet slowly to avoid bloating.
*Getting plenty to drink. Drinking eight 8-ounce glasses of liquid a day may help prevent constipation. Water is a good choice. You should avoid drinks with caffeine, alcohol, milk, or carbonation if they give you diarrhea.
*Kegel exercise or pelvic floor exercise is very much useful. This exercise
consists of repeatedly contracting and relaxing the muscles that form part of the pelvic floor, now sometimes colloquially referred to as the “Kegel muscles”. The exercise needs to be performed multiple times each day, for several minutes at a time, for one to three months, to begin to have an effect.
[amazon_link asins=’B014GMBDQ2,B01FQ21X16,B01LX505AF,B01EL6A6IO,B01N5HE16R,B00W6T35J6,B018IFNSX4,B01KIKW4LO,B01H14XXP6′ template=’ProductCarousel’ store=’finmeacur-20′ marketplace=’US’ link_id=’589139f6-0b93-11e7-b70e-3fd40db10f88′]
MEDICATIONS:
In people with bowel incontinence due to diarrhea, medications such as loperamide (Imodium) may be used to control the diarrhea and improve bowel incontinence.
Other antidiarrheal medications include anti-cholinergic medications (belladonna or atropine), which reduce intestinal secretions and movement of the bowel. Opium derivatives (paregoric or codeine) or diphenoxylate (lomotil), as well as loperamide (Imodium) increase intestinal tone and decrease movement of the bowel.
Other medications used to control bowel incontinence include drugs that reduce water content in the stools (activated charcoal or Kaopectate) or that absorb fluid and add bulk to the stools (Metamucil).
MEDICATION EVALUATION: With your health care provider, review all the medications you take. Certain medications can cause or increase bowel incontinence, especially in older people. These medications include:
*Antacids
*Laxatives
OTHER THERAPIES:
If you often have bowel incontinence, you can use special fecal collection devices to contain the stool and protect your skin from breakdown. These devices consist of a drainable pouch attached to an adhesive wafer. The wafer has a hole cut through the center, which fits over the opening to the anus.
Most people who have bowel incontinence due to a lack of sphincter control, or decreased awareness of the urge to defecate, may benefit from a bowel retraining program and exercise therapies to help restore normal muscle tone.
Special care must be taken to maintain bowel control in people who have a decreased ability to recognize the urge to defecate, or who have impaired mobility that prevents them from independently and safely using the toilet. Such people should be assisted to use the toilet after meals, and promptly helped to the toilet if they have the urge to defecate.
If toileting needs are often unanswered, a pattern of negative reinforcement may develop. In this case people no longer take the correct actions when they feel the urge to have a bowel movement
You may click & See : Toileting safety
SURGERY
People who have bowel incontinence that continues even with medical treatment may benefit from surgery to correct the problem. Several different options exist. The choice of surgery is based on the cause of the bowel incontinence and the person’s general health.
RECTAL SPHINCTER REPAIR
Sphincter repair is performed on people whose anal muscle ring (sphincter) isn’t working well due to injury or aging. The procedure consists of re-attaching the anal muscles to tighten the sphincter and helping the anus close more completely.
GRACILIS MUSCLE TRANSPLANT
In people who have a loss of nerve function in the anal sphincter, gracilis muscle transplants may be performed to restore bowel control. The gracilis muscle is taken from the inner thigh. It is put around the sphincter to provide sphincter muscle tone.
ARTIFICIAL BOWEL SPHINCTER
Some patients may be treated with an artificial bowel sphincter. The artificial sphincter consists of three parts: a cuff that fits around the anus, a pressure-regulating balloon, and a pump that inflates the cuff.
The artificial sphincter is surgically implanted around the rectal sphincter. The cuff remains inflated to maintain continence. You have a bowel movement by deflating the cuff. The cuff will automatically re-inflate in 10 minutes.
FECAL DIVERSION
Sometimes a fecal diversion is performed for people who are not helped by other therapies. The large intestine is attached to an opening in the abdominal wall called a colostomy. Stool passes through this opening to a special bag. You will need to use a colostomy bag to collect the stool most of the time.
Regular Yoga exercise & Meditation under the supervision of an expart will defenitely help a lot to get rid of the problem.
Disclaimer: This information is not meant to be a substitute for professional medical advise or help. It is always best to consult with a Physician about serious health concerns. This information is in no way intended to diagnose or prescribe remedies.This is purely for educational purpose.
Resources:
http://www.niddk.nih.gov/health-information/health-topics/digestive-diseases/bowel-control/Pages/ez.aspx
http://www.nlm.nih.gov/medlineplus/ency/article/003135.htm
















![Reblog this post [with Zemanta]](https://i0.wp.com/img.zemanta.com/reblog_e.png?w=580)










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}