Definition:
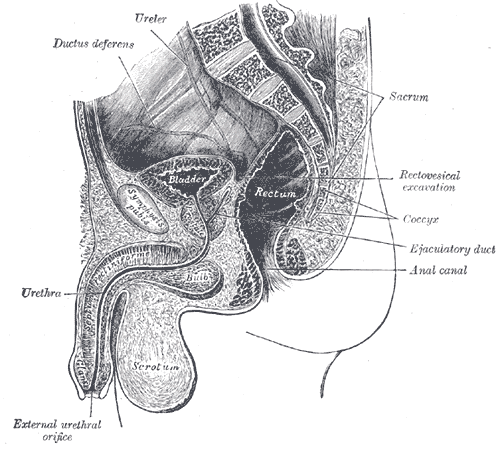
The spleen is a soft plum-coloured organ, packed with blood-filled tissues and covered by a smooth membrane. It’s located in the abdomen just beneath the left side of the diaphragm, under the ribs, and is shaped like a loosely clenched fist. CLICK & SEE THE PICTURES
The spleen’s vulnerable location and softness means it’s at risk of injury. A severe blow to the stomach area can squash the spleen, splitting or tearing its covering membrane and the tissue inside and allowing blood to rapidly leak out – rather like a squashed tomato.
A ruptured spleen is a serious condition that can occur when your spleen experiences a trauma. With enough force, a blow to your abdomen — during a sporting mishap, a fistfight or a car crash, for example — might lead to a ruptured spleen. Without emergency treatment, a ruptured spleen can cause life-threatening internal bleeding.
Though some ruptured spleens require emergency surgery, others with ruptured spleens can be treated with several days of hospital care.
Symptoms
The abdomen usually feels tender and painful when the spleen ruptures. Blood leaks into the abdomen, causing irritation with subsequent tenderness and pain. Classically, a patient with a ruptured spleen describes feeling left shoulder-tip pain (this pain comes from irritation of the diaphragm by the spilt blood).
If the leak of blood is gradual, symptoms may not occur until the blood supply to the body is diminished. This will result in low blood pressure and light-headedness, blurred vision, confusion and loss of consciousness, as the oxygen supply to the heart and brain is affected. If blood loss is rapid, the person may suddenly collapse.
Causes:
A ruptured spleen is the most common serious complication of an abdominal injury and may occur as a consequence of road traffic accidents, sports injuries and violent, physical attacks.
*Injury to the left side of the body. A ruptured spleen is typically caused by a blow to the left upper abdomen or the left lower chest, such as might happen during sporting mishaps, fistfights and car crashes.
*An injured spleen may rupture soon after the abdominal trauma or, in some cases, days or even weeks after the injury.An enlarged spleen. Your spleen can become enlarged when blood cells accumulate in the spleen. An enlarged spleen can be caused by various underlying problems, such as mononucleosis and other infections, liver disease and blood cancers.
Complications: A ruptured spleen can cause life-threatening bleeding into your abdominal cavity.
Diagnosis:
Normal procedures to diagnose a ruptured spleen include:
*A physical exam. During a physical exam doctor will use his or her hands to place pressure on your abdomen to determine the size of your spleen and whether you’re experiencing any abdominal tenderness.
*Drawing fluid from abdomen. The Doctor may use a needle to draw a sample of fluid from the abdomen. If the sample reveals blood in the abdomen, the patient may be referred for emergency treatment.
*Imaging tests of the abdomen. If your diagnosis isn’t clear, the doctor may recommend an abdominal computerized tomography (CT) scan or another imaging test to identify or rule out other possible causes as per symptoms.
Treatment :
Untreated, a ruptured spleen can be rapidly fatal, so it requires urgent medical and surgical treatment.
Fluids must quickly be given through an intravenous drip in order to maintain the circulation to the organs of the body (including a blood transfusion) and emergency surgery is performed to stop the leak of blood.
Sometimes, if the rupture is only small, it’s possible for the surgeon to repair the spleen. However, usually the entire spleen needs to be removed in an operation called a splenectomy.
The spleen plays an important part in protecting the body against infection. In particular it clears a type of bacteria known as pneumococcus from the body. So it’s important that those who’ve had their spleen removed take extra precautions to protect themselves against infection. In particular, they should be vaccinated against pneumococcal infection.
Prognosis: Splenic rupture permits large amounts of blood to leak into the abdominal cavity, possibly resulting in shock and death. Patients typically require emergency surgery, although it is becoming more common to simply monitor the patient to make sure the bleeding stops by itself and to allow the spleen to heal itself. Rupture of a normal spleen can be caused by trauma, for example, in an accident. If an individual’s spleen is enlarged, as is frequent in mononucleosis, most physicians will not allow activities (such as contact sports) where injury to the abdomen could be catastrophic.
Prevention
The spleen is a useful organ and it is essential to life. It is sometimes removed (splenectomy) in those who have blood disorders, such as thalassemia or hemolytic anemia. If the spleen is removed, a person must receive certain immunizations to help prevent infections that the spleen normally fights.
Disclaimer: This information is not meant to be a substitute for professional medical advise or help. It is always best to consult with a Physician about serious health concerns. This information is in no way intended to diagnose or prescribe remedies.This is purely for educational purpose.
Definition:
Reye’s syndrome is a potentially fatal disease that causes numerous detrimental effects to many organs, especially the brain and liver, as well as causing a lower than usual level of blood sugar (hypoglycemia).. Reye’s syndrome most often affects children and teenagers recovering from a viral infection and who may also have a metabolic disorder. The exact cause is unknown, and while it has been associated with aspirin consumption by children with viral illness, it also occurs in the absence of aspirin use.
.You may click to see larger picture
The disease causes fatty liver with minimal inflammation and severe encephalopathy (with swelling of the brain). The liver may become slightly enlarged and firm, and there is a change in the appearance of the kidneys. Jaundice is not usually present.
Early diagnosis is vital; while most children recover with supportive therapy, severe brain injury or death are potential complications.
Boys and girls can both be affected, but the condition is very rare – there were only three reported cases in the UK and Ireland in 2000.
The syndrome is named after Dr. R. Douglas Reye, who, along with fellow physicians Dr. Graeme Morgan and Dr. Jim Baral, published the first study of the syndrome in 1963 in The Lancet. In retrospect, the occurrence of the syndrome may have first been reported in 1929.
Symptoms :
Reye’s syndrome progresses through five stages, explained below:
*Stage I
…#Rash on palms of hands and feet
…#Persistent, heavy vomiting that is not relieved by not eating
…#Generalized lethargy
…#Confusion
…#Nightmares
…#High fever
…#Headaches
*Stage II
…#Stupor caused by encephalitis
…#Hyperventilation
…#Fatty liver (found by biopsy)
…#Hyperactive reflexes
*Stage III
…#Continuation of Stage I and II symptoms
…#Possible coma
…#Possible cerebral oedema
…#Rarely, respiratory arrest
*Stage IV
…#Deepening coma
…#Dilated pupils with minimal response to light
…#Minimal but still present hepatic dysfunction
*Stage V
…#Very rapid onset following stage IV
…#Deep coma
…#Seizures
…#Multiple organ failure
…#Flaccidity
…#Hyperammonemia (above 300 mg/dL of blood)
…#Death
Causes:
The cause of Reye’s syndrome isn’t fully understood. Reye’s syndrome seems to be triggered by using aspirin to treat a viral illness or infection — particularly flu (influenza) and chickenpox — in children and teenagers who have an underlying fatty acid oxidation disorder. Fatty acid oxidation disorders are a group of inherited metabolic disorders in which the body is unable to breakdown fatty acids because an enzyme is missing or not working properly. A screening test is needed to determine if your child has a fatty acid oxidation disorder.
In some cases, Reye’s syndrome may be an underlying metabolic condition that’s unmasked by a viral illness. Exposure to certain toxins — such as insecticides, herbicides and paint thinner — also may contribute to Reye’s syndrome.
Risk Factors:
The following factors — usually when they occur together — may increase your child’s risk of developing Reye’s syndrome:
Using aspirin to treat a viral infection, such as flu, chickenpox or an upper respiratory infection
Having an underlying fatty acid oxidation disorder
Complications:
Most children and teenagers who have Reye’s syndrome survive, although varying degrees of permanent brain damage are possible. Without proper diagnosis and treatment, Reye’s syndrome can be fatal within a few days.
Diagnosis:
Exams and TestsThe following tests may be used to diagnose Reye syndrome:
•Blood chemistry tests
•Head CT or head MRI scan
•Liver biopsy
•Liver function tests
•Serum ammonia test
•Spinal tap
Treatment:
Immediate emergency treatment is needed for Reye’s syndrome, usually in an intensive care unit.
There is no specific treatment for this condition. The health care provider will monitor the pressure in the brain, blood gases, and blood acid-base balance (pH).
Treatments may include:
•Breathing support (a breathing machine may be needed during a deep coma)
•Fluids by IV to provide electrolytes and glucose
•Steroids to reduce swelling in the brain
Prognosis :
Documented cases of Reye’s syndrome in adults are rare. The recovery of adults with the syndrome is generally complete, with liver and brain function returning to normal within two weeks of the illness. In children, however, mild to severe permanent brain damage is possible, especially in infants. Over thirty percent of the cases reported in the United States from 1981 through 1997 resulted in fatality.
Disclaimer: This information is not meant to be a substitute for professional medical advise or help. It is always best to consult with a Physician about serious health concerns. This information is in no way intended to diagnose or prescribe remedies.This is purely for educational purpose.
Definition:
Over a lifetime, it’s estimated the human gut digests more than 65 tonnes of food and drink. Much of this food will be low in fibre, putting the gut under strain.
One common outcome of this is diverticular disease, a condition affecting the large bowel, or colon, believed to be the result of too little fibre in the diet.
A diet low in fibre creates the ideal conditions for constipation to develop. When this happens, the pressure in the large part of the gut increases, which forces small parts of the gut lining outwards through the muscles surrounding the gut. This causes the lining to form small balloon-like pouches called diverticula..
Author: U.S. National Institute of Diabetes and Digestive and Kidney Disease (NIDDK), National Institutes of Health (NIH) Source URL: http://win.niddk.nih.gov/publications/gastric.htm Copyright tag: Why? Because it’s from an NIH department. Category:Obesity images (Photo credit: Wikipedia)
Diverticula are pockets that develop in the colon wall, usually in the sigmoid or left colon, but may involve the entire colon. Diverticulosis describes the presence of these pockets. Diverticulitis describes inflammation or complications of these pockets.
About one in two adults over 50 is affected, and most adults are affected by the time they reach 80 to 90. Men and women are affected equally.
Diverticular disease is very uncommon in countries such as Africa, where diets are high in fibre. In Western countries, where many people still don’t eat enough fibre, it becomes more common as people get older.
Symptoms:
Signs and symptomsMost people with colonic diverticulosis are unaware of this structural change. When symptoms do appear in a person over 40 years of age it is important to obtain medical advice and exclude more dangerous conditions such as cancer of the colon or rectum.
The clinical forms of colonic diverticulosis are
*Symptomatic colonic diverticulosis………..click to see the picture
This is the most common complication of colonic diverticulosis. This is when the motility (that is, the onward propulsive nature of contractions) of the bowel becomes disorganized. Sometimes, spasm can develop. This results in pain in the left lower abdomen and often is accompanied by the passage of small pelletty stools and slime which relieves the pain. Symptoms can consist of (1) bloating, (2) changes in bowel movements (diarrhea or constipation), (3) Non-specific chronic discomfort in the lower left abdomen, with occasional acute episodes of sharper pain, (4) abdominal pain, often aftick to see the pictureer meals often in the left lower abdomen. If these persist clinical investigation is advised.
*Complicated colonic diverticulosis
This is very uncommon but highly dangerous. The diverticulae may bleed, either rapidly (causing bleeding through the rectum) or slowly (causing anaemia). The diverticulae can become infected and develop abscesses, or even perforate. These are serious complications and medical care is needed. Infected diverticulae and development of abscesses merits the term diverticulitis. First time bleeding from the rectum, especially in individuals aged over age 40, could be due to colon cancer, colonic polyps and inflammatory bowel disease rather than diverticulosis and requires clinical investigation.
Infection in the diverticula, possibly caused by an impacted piece of faeces, is responsible for the inflammation that develops. When this happens – called diverticulitis – the pain is very severe and usually felt in the lower left side of the abdomen.
A person will often feel feverish and have nausea and vomiting. They may pass blood rectally.
Risk factors:
1.increasing age
2.constipation
3.a diet that is low in dietary fiber content or high in fat
4.high intake of meat and red meat
5.connective tissue disorders (such as Marfan syndrome) that may cause weakness in the colon wall.
The exact aetiology of colonic diverticulosis has yet to be fully clarified and many of the claims are only anecdotal. The modern emphasis on the value of fiber in the diet began with Cleave. A strong case was made by Neil Painter and Adam Smith that a deficiency of dietary fiber is the cause of diverticular disease. They argued that the colonic muscles needed to contract strongly in order to transmit and expel the small stool associated with a fiber deficient diet. The increased pressure within the segmented section of bowel over years gave rise to herniation at the vulnerable point where blood vessels enter the colonic wall. Denis Burkitt had suggested that the mechanical properties of the colon may be different in the African and the European subjects. Because Africans eat a diet containing much more fiber than Europeans and use the natural squatting position for defecation, they pass bulky stools, and hence rarely if ever develop colonic diverticulosis. The US National Institutes of Health (NIH) considers the fiber theory “unproven.”
However, change in the strength of the colonic wall with age may be an aetiological factor. Connective tissue is a significant contributor to the strength of the colonic wall. The mechanical properties of connective tissue depend on a wide variety of factors, the type of tissue and its age, the nature of the intramolecular and intermolecular covalent cross links and the quantity of the glycosaminoglycans associated with the collagen fibrils. The submucosa of the colon is composed almost entirely of collagen, both type I and type III. Several layers of collagen fibres make up the submucosa of the human colon. The collagen fibril diameters and fibril counts are different between the left and right colon and change with age and in colonic diverticulosis,. The implication being that changes which are normally associated with ageing are more pronounced in colonic diverticulosis. Iwasaki found that the tensil strength of the Japanese colon obtained at postmortem declined with age. Similarly the mechanical properties of the colon are stronger in African than European subjects. However, this race-based claim is contradicted by the virtually identical incidence of diverticular disease in black and white Americans.
The strength of the colon decreases with age in all parts of the colon, except the ascending colon. The fall in tensile strength with age is due to a decrease in the integrity of connective tissue. Cross linkage of collagen is increased in colonic diverticulosis. The mucosal layer is possibly more elastic and it is likely that the stiffer external layers break and allow the elastic mucosa to herniate through forming a diverticulum. Collagen has intermolecular and intramolecular cross links which stabilise and give strength to the tissue in which it is located. Accumulation of covalently linked sugar molecules and related increasing cross linking products are found in a variety of tissues with ageing, skin, vascular tissue, the cordae tendinae of heart valves and the colon. This reduces the strength and pliability of the collagen. Colonic diverticulosis increases in frequency with age. There is a reduction in the strength of the colonic mucosa with age, and that increased contractions in the descending and sigmoid colon secondary to an insufficient fibre content of the diet cause protrusion through this weakened wall. Colonic diverticulosis is in general a benign condition of the bowel which uncommonly becomes symptomatic and even less commonly becomes a truly clinical complicated problem.
Diagnosis:
In cases of asymptomatic Diverticulosis, the diagnosis is usually made as an incidental finding on other investigations.
While a good history is often sufficient to form a diagnosis of Diverticulosis or Diverticulitis, it is important to confirm the diagnosis and rule out other pathology (notably colorectal cancer) and complications.
Investigations:-
*Plain Abdominal X-ray may show signs of a thickened wall, ileus, constipation, small bowel obstruction or free air in the case of perforation. Plain X-rays are insufficient to diagnose Diverticular Disease.
*Contrast CT is the investigation of choice in acute episodes of Diverticulitis and where complications exist.
*Colonoscopy will show the diverticulum and rule out malignancy. A Colonoscopy should be performed 4–6 weeks after an acute episode.
*Barium enema is inferior to colonoscopy in terms of image quality and is usually only performed if the patient has strictures or an excessively tortuous sigmoid colon where colonoscopy is difficult or dangerous.
*MRI provides a clear picture of the soft tissue of the abdomen, however its expense often outweighs the benefits when compared to contrast CT or colonoscopy.
*There is no blood test for Diverticulosis.
It is important to note that both Barium enema and Colonoscopy are contraindicated during acute episodes of diverticulitis.
Management & Treatment:
Many patients with diverticulosis have minimal or no symptoms, and do not require any specific treatment. A high-fiber diet and fiber supplements are advisable to prevent constipation . The American Dietetic Association recommends 20-35 grams each day. Wheat bran has much to commend it as this has been shown to reduce intra colonic pressure Ispaghula is also effective at 1-2 grams a day. Colonic stimulants should be avoided. The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) says foods such as nuts, popcorn hulls, sunflower seeds, pumpkin seeds, caraway seeds, and sesame seeds have traditionally been labelled as problem foods for people with this condition; however, no scientific data exists to prove this hypothesis. The seeds in tomatoes, zucchini, cucumbers, strawberries, raspberries, and poppy seeds, are not considered harmful by the NIDDK. Treatments, like some colon cleansers, that cause hard stools, constipation, and straining, are not recommended. Some doctors also recommend avoidance of fried foods, nuts, corn, and seeds to prevent complications of diverticulosis. Whether these diet restrictions are beneficial is uncertain; recent studies have stated that nuts and popcorn do not contribute positively or negatively to patients with diverticulosis or diverticular complications. When the spasm pain is troublesome the use of peppermint oil (1 drop in 50 ml water), or peppermint tablets (e.g., colpermin), can be helpful. Complicated diverticulosis requires treatment of the complication. These complications are often grouped under a single diagnosis of diverticulitis and require skilled medical care of the infection, bleeding and perforation which may include intensive antibiotic treatment, intravenous fluids and surgery. Complications are more common in patients who are taking NSAIDS or aspirin. As diverticulosis occurs in an older population such complications are serious events.
Someone with diverticulitis may be treated at home with painkillers, antibiotics, laxatives and dietary advice. But diverticulitis is often severe, and can need hospital treatment with antibiotics and fluids given through a drip.
In some cases, the bowel may perforate, become obstructed or bleed heavily. When this happens, the situation becomes an emergency and an operation may be needed.
Surgery is reserved for patients with recurrent episodes of diverticulitis, complications or severe attacks when there’s little or no response to medication. Surgery may also be required in individuals with a single episode of severe bleeding from diverticulosis or with recurrent episodes of bleeding.
Surgical treatment for diverticulitis removes the diseased part of the colon, most commonly, the left or sigmoid colon. Often the colon is hooked up or “anastomosed” again to the rectum. Complete recovery can be expected. Normal bowel function usually resumes in about three weeks. In emergency surgeries, patients may require a temporary colostomy bag. Patients are encouraged to seek medical attention for abdominal symptoms early to help avoid complications.
Complications:
Infection of a diverticulum can result in diverticulitis. This occurs in 10-25% of persons with diverticulosis (NIDDK website). Tears in the colon leading to bleeding or perforations may occur; intestinal obstruction may occur (constipation or diarrhea does not rule this possibility out); and peritonitis, abscess formation, retroperitoneal fibrosis, sepsis, and fistula formation are also possible occurrences. Rarely, an enterolith may form.
Low fiber, high fat diet, constipation and use of stimulant laxatives increase the risk of bleeding, also history of diverticulitis increases the chance to bleed.
Infection of a diverticulum often occurs as a result of stool collecting in a diverticulum.
More than 10% of the US population over the age of 40 and half over the age of 60 has diverticulosis. This disease is common in the US, Britain, Australia, Canada, and is uncommon in Asia and Africa . Large-mouth diverticula are associated with scleroderma.
Disclaimer: This information is not meant to be a substitute for professional medical advise or help. It is always best to consult with a Physician about serious health concerns. This information is in no way intended to diagnose or prescribe remedies.This is purely for educational purpose.
Definition:
Anal stenosis refers to a narrowing of the anal opening, which makes it difficult for stool contents to pass through easily. Symptomatic children tend to be particularly colicky babies, because of the discomfort associated with the stool backing up. The stool may exit under pressure and look almost like a squirt gun. Treatment of this disorder usually involves gentle dilation of the anal opening. This is typically done twice a day. Every week a slightly larger lubricated dilator is passed to stretch the anus until it reaches normal size. In very mild cases, softening the stool may be sufficient until the anus grows sufficiently. Suppositories can make the child comfortable in the short run, but do run the risk of dependence. At around 4 months, apple or even prune juice may help the child to pass stool. Rarely, surgery is needed to insure an opening of adequate caliber. If this is an isolated anomaly, the prognosis is excellent.
You may click to see the picture
Some children are born with no anal opening at all. This is called an imperforate anus. The rectum ends in a blind pouch, about 2 cm inside the perianal skin. Usually the sphincters are well developed. For these children, a colostomy is indicated during the newborn period, but once the final surgery corrects the defect, the prognosis is likewise excellent.
The most frequent anorectal defect seen in boys is the recto-urethral fistula, or a communication between the rectum and the lower part of the urethra. These children also require a colostomy before the definitive repair period. The long term prognosis for normal urethral and rectal function is good.
Scar formation after perianal fistulae, trauma, severe anal sac disease, or treatment for neoplasia may result in a reduced lumen and particularly a loss of the capacity to dilate with passage of feces. Straining, passage of ribbon-like feces and constipation result.
Symptoms
The restriction of the anal canal prevents the normal expulsion of faeces, resulting in difficulty and pain when trying to open the bowels, and leading to constipation. Babies may also experience pain when trying to open their bowels.
Causes and risk factors:
Anal stenosis may be present from birth, when it might be accompanied by malformations of the anal opening. This happens in one in several thousand births.
Sometimes the opening appears further forward than normal. In girls, it’s usually immediately behind or inside the female genitalia. In boys, there may be no obvious opening at all or just a small area of bulging skin or a tiny channel under the skin.
More commonly, stenosis develops as a result of scarring from a tiny fissure, or crack, in the anal canal. This is usually the reason why adults develop anal stenosis, but it can also occur in babies.
Anal stenosis may also develop after surgery to the anus, for example after the removal of piles or haemorrhoidectomy.
Treatment and recovery: Low-risk treatments:
Laxatives, suppositories and other treatments are used to help loosen motions and lubricate the anal canal, to make it easier to empty the bowels. There’s little risk the person affected will come to any harm from these treatments if they’re used as prescribed and only for a matter of months while the problem settles. (It must be remembered that the risks are considerably less than those that might occur if the affected person becomes very constipated).
One solution to this problem is to simply insert a plastic tube known appropriately as an “anoscope” and relieve the obstruction. ..You may click to see the picture.
Individuals suffering from anal stenosis aren’t likely to become dependent on the laxatives and suppositories.
However, its also important to make dietary changes (such as plenty of raw fruit and vegetables to provide natural fibre, and plenty of fluid to avoid dehydration) in order to keep the motions soft. Regular exercise also helps keep a regular bowel habit.
Surgical treatments:
In mild cases, gentle and gradual dilation by the regular passage of normal motions may be enough. But quite often surgery is needed, especially in more severe cases. The surgical treatment of anal stenosis depends on the extent of the problem. In most cases all that’s needed is for the anal canal to be stretched. Often this can be done by the doctor in the hospital clinic, without the need for anaesthetic.
If the stenosis is severe, dilation may performed under anaesthesia. More major surgery is only needed if the anal canal needs reconstructing or (in small children with congenital anal stenosis) it needs repositioning or there are other malformations that require surgery.
Disclaimer: This information is not meant to be a substitute for professional medical advise or help. It is always best to consult with a Physician about serious health concerns. This information is in no way intended to diagnose or prescribe remedies.This is purely for educational purpose.
For people with chronic heartburn, too much running and jumping can induce acid reflux. However, the right type of exercise may actually improve the condition.
“The specific exercise is crucial. Scientists found that aerobic exercises with the highest ‘agitation of the body,’ like vigorous running, consistently induced acid reflux, even in people who did not have chronic heartburn …
Another factor is body position. Bench presses, leg curls or any other exercise that involves lying flat sharply raise the risk of acid reflux.”
What Types of Activities Make Heartburn Worse?
As you might suspect, vigorous jumping, bouncing, running and other activities that cause agitation of your body can make heartburn worse, simply because it makes it easier for your stomach acid to move into your esophagus. For this reason, vigorous aerobics and other agitating exercise routines may exacerbate your symptoms, especially if you eat within two hours of your workout.
That said, heartburn also tends to flare up during other routine activities as well, such as:
•After eating a heavy meal
•Bending over
•Lifting
•Lying down, especially when laying on your back
If you know you have GERD, or even if you suffer from heartburn only occasionally, it makes sense to limit these activities, especially shortly after eating, or at least tailor them so they’re less likely to cause a problem.
For instance, by eating smaller portions at your meals it can help you to avoid overeating, which is a major trigger for heartburn. Likewise, if you wait two or three hours after dinner before lying down in bed, it will also give you some relief.
When you do lie down, elevating the head of your bed may make you more comfortable, as can squatting down when you need to pick something up (instead of bending over).
And just as you can modify these common activities so they don’t make your heartburn worse, you can modify your exercise program to follow suit as well.
But at the same time Exercise is Essential, Even if You Have Heartburn
One of my top recommendations for treating heartburn and GERD is to implement an exercise program.
Physical activity is an important way to improve your body’s immune system, which is imperative to fight off all kinds of infections. What does this have to do with GERD?









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}